|
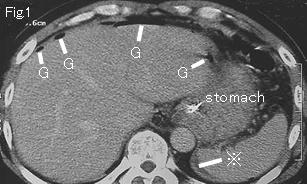
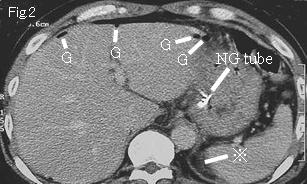
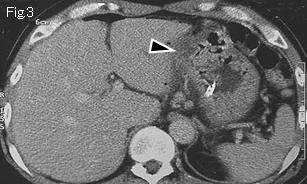
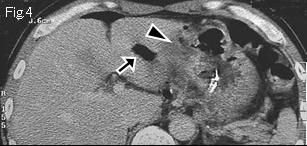
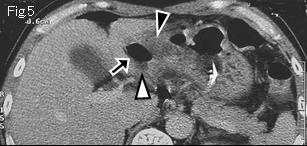
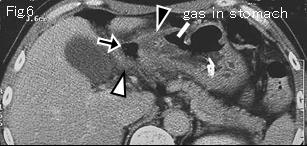
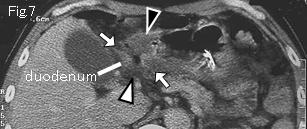
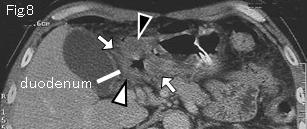
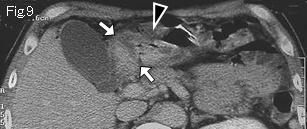
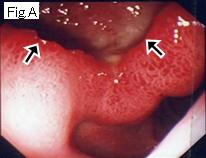
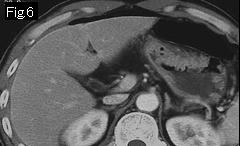
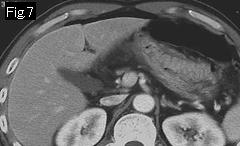
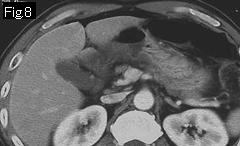
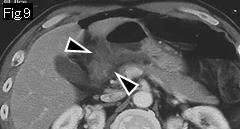
Fig.1 and Fig.2 show ascites (reference mark) and free air (G). Anterior wall of antrum demonstrates edematous wall thickening (black arrowhead) from gastric angle in Fig.3-Fig.9, but no obvious ulcerative lesion. Duodenal bulb is shown in Fig.7 and Fig.8, and white arrow indicates pyloric ring. The wall of duodenal bulb is thickened with submucosal edema (white arrowhead). Gas (black arrows) of Fig.4-Fig.6 connects to duodenal bulb lumen, and is projecting to the outside of bulb, suggesting being an acute ulcer because it is associated with edematous wall (white arrowhead) in Fig.5 and Fig.6. Because of small amount of ascites on CT scan, the patient was treated conservatively with success. Endoscopy one week later revealed a large active duodenal ulcer (Fig.A: black arrow) that is consistent with CT findings.
|
|
Reference case: (5mm slice, duodenal ulcer perforation): A 47-year-old male without history of peptic ulcer, had right upper quadrant pain for three days. He presented with sudden onset of intense epigastric pain during driving. Temperature: 36.0 degrees Celsius. Signs of peritoneal irritation were shown in the entire abdomen.
|
|
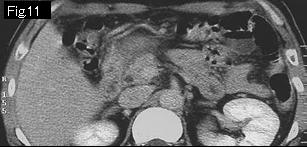
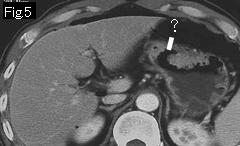
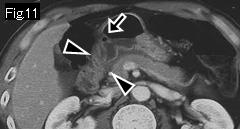
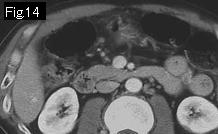
Because there seems to be no acute lesion in stomach, attention should be paid to duodenum. ? of Fig.5 is not an acute ulcer, because there is no associated edematous wall thickening around it. Duodenal bulb shows edematous wall thickening (black arrowheads) in Fig.9-Fig.12, and a small gas (black arrow) of Fig.10 and Fig.11 is suggestive of an acute ulcer. In presence of free air and ascites, edematous wall of duodenal bulb is highly indicative of duodenal ulcer perforation despite a lack of recognizable ulcerative lesion. Perforated acute ulcer of anterior wall of duodenal bulb was confirmed by surgery (Fig.B: white arrow).
|
|