|
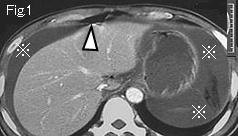
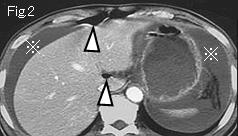
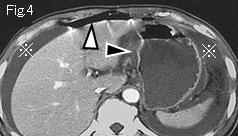
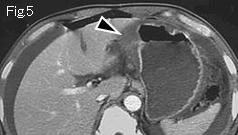
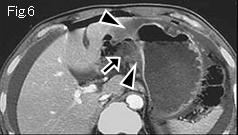
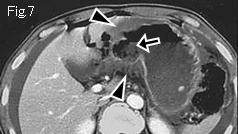
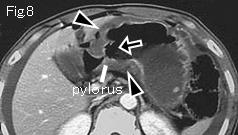
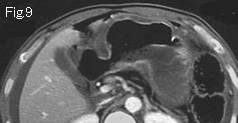
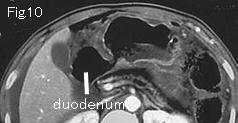
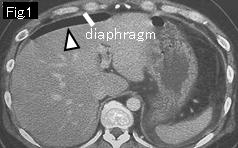
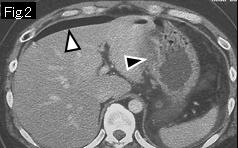
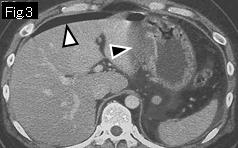
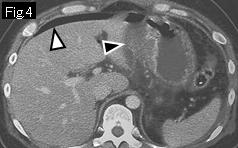
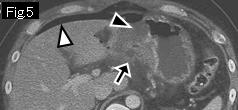
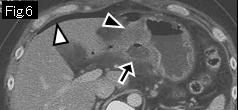
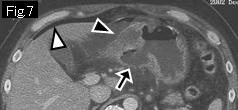
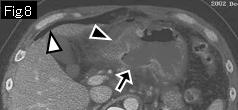
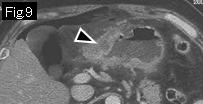
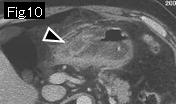
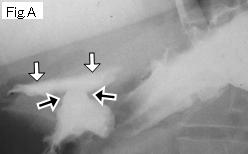
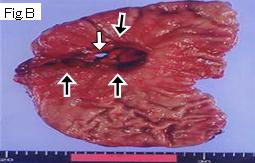
Reference Case (perforated gastric ulcer): A 37-year-old male with a past history of duodenal ulcer at age of 17 years, developed moderate epigastric pain for a week. The pain suddenly became severe, and he presented to ER because of no improvement over 8 hours. Temperature: 38.7 degrees Celsius. On physical examination, board-like rigidity was noted in epigastrium. There is free air (white arrowhead), wall thickening by submucosal edema (black arrowhead), and black arrow is an acute ulcerative lesion. Gastrografin contrast study of Fig.A showed a gastric ulcer (black arrows) and leakage (white arrows) of contrast medium into free peritoneal cavity. Operative and pathologic finding: benign ulcer perforation (Fig.A: black arrows. White arrow is perforation site).
|