|
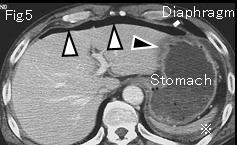
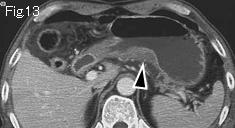
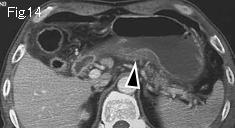
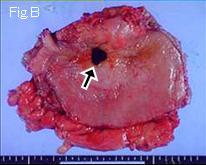
Free air (white arrowheads) and ascitic fluid (Fig.5-Fig.8: reference mark) strongly suggest gastrointestinal perforation. In many cases, it is possible to diagnose and differentiate gastric from duodenal ulcer perforation. Edematous thickening of stomach wall extends from lesser curvature of stomach (Fig.5: black arrowhead) to posterior wall (Fig.14). A defect in thickened edematous wall (Fig.8-Fig12: black arrow) indicates an acute ulcerative lesion. Thin (5mm) slice images facilitate diagnosis of gastric ulcer perforation in this case. As black arrows of Fig.8 and Fig.9 show, the base of deep ulcer at gastric angle is usually seen at a distant site from the gastric wall. The upper GI series show leakage of large amount of contrast medium (Fig.A: white arrows). Laparotomy confirmed above findings (black arrow of Fig.B is perforated gastric ulcer).
|