|
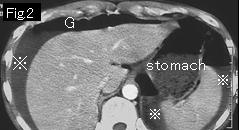
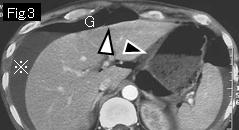
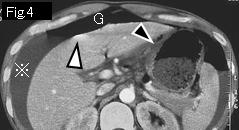
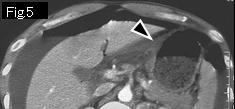
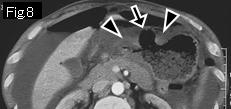
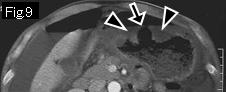
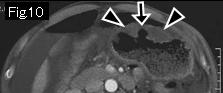
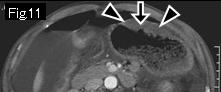
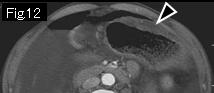
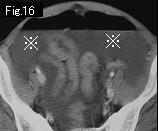
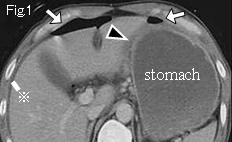
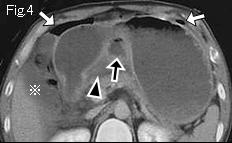
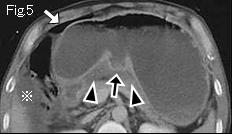
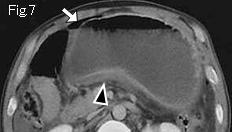
Presence of massive ascitic fluid (reference mark), free air (G), edematous wall thickening at lesser curvature of stomach (Fig.3: black arrowheads), and an ulcerative lesion extending from gastric angle to anterior wall of stomach (Fig.6–Fig.11: black arrows) are indicative of gastric ulcer perforation. Foamy gas (white arrows) of Fig.17 should be considered as food debris (leaked intestinal content). S: sigmoid colon. Upper GI series shows a giant gastric ulcer (Fig.A: white arrowhead). Laparotomy revealed perforated gastric ulcer(2cm in size) at anterior wall of stomach.
|