|
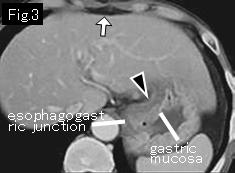
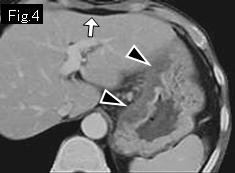
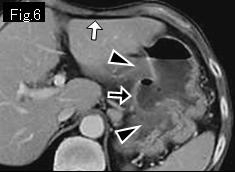
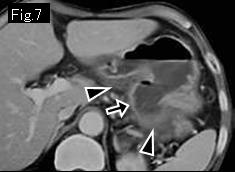
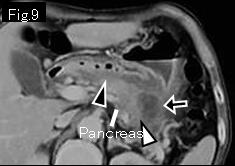
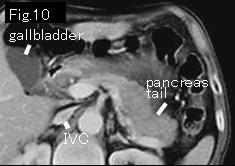
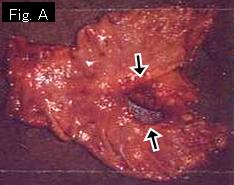
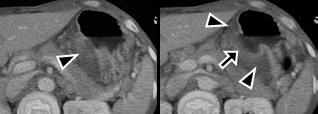
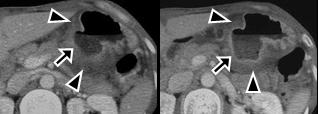
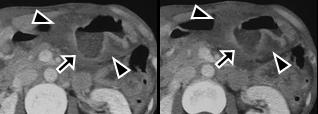
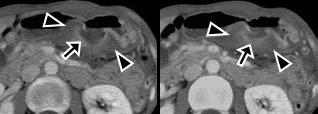
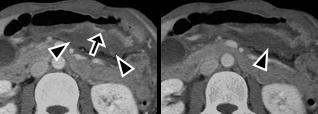
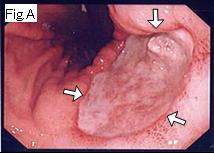
White arrows of Fig.3-Fig.6 are not gas but adipose tissue. Because of absence of any free air (pneumoperitoneum) and ascitic fluid, possibility of gastrointestinal perforation is very unlikely. Fig.3 shows low density (water density) layer (black arrowheads) indicating thickening of gastric wall (>2 cm) due to submucosal edema. Fig.5-Fig.9 depict circular defect (black arrow) in gastric wall. This defect is the ulcerative lesion which extends from gastric angle to posterior wall. Acute gastric ulcers are always accompanied by surrounding submucosal edema. A diagnosis of the acute ulcerative lesion of stomach could easily be made by identifying edematous thickening of wall (black arrowheads of Fig.3-Fig.9) and circular wall defect (Fig.5-Fig.9: black arrow). The base of the ulcer penetrates into the pancreas (Fig.9: white arrowhead) as indicated by edematous pancreatic tail. A smaller IVC than the aorta just above confluence of renal vein in Fig.10 suggests moderate hypovolemia. Endoscopy revealed a large gastric ulcer which penetrated into the pancreas. Because of poor response to conservative treatment, the subtotal gastrectomy was performed. Fig.A shows the penetrating gastric ulcer (black arrow). Pathologic diagnosis: perforated, benign gastric ulcer.
|